Table of Contents
Q What is plantar fasciitis?
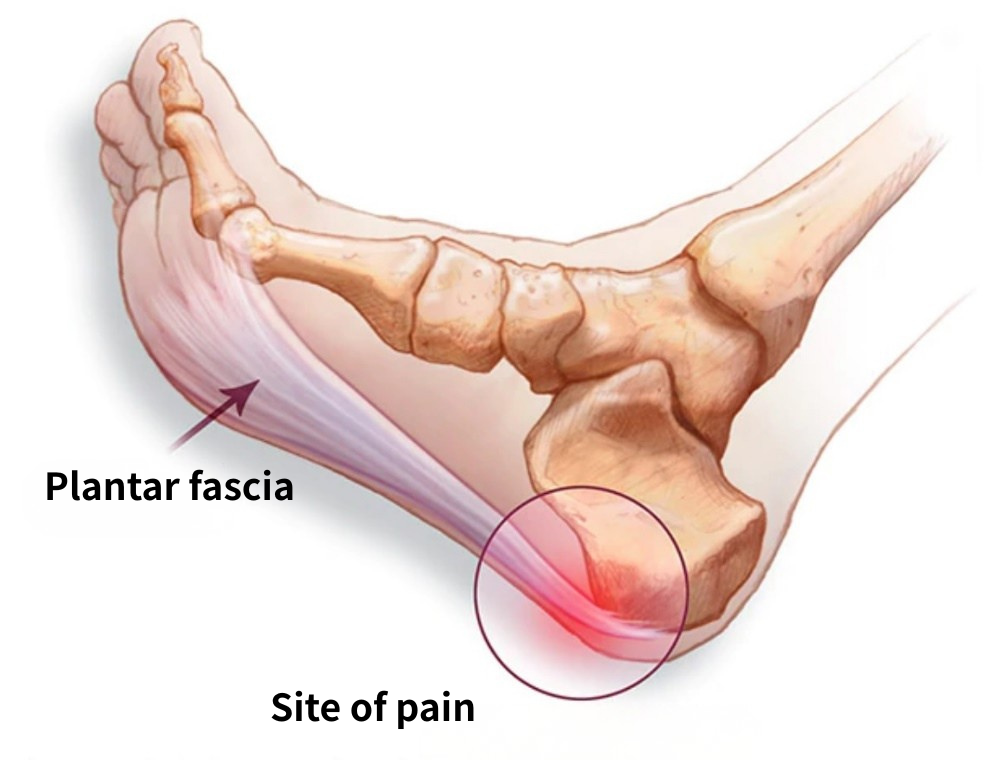
Plantar fasciitis is the most common cause of heel pain. The plantar fascia is a thick band of tissue that runs along the sole of the foot from the toes to the heel. Plantar fasciitis is inflammation at the point where this fascia attaches to the heel bone, known as the insertion site. A characteristic feature of the condition is sharp pain in the heel with the very first step taken upon getting out of bed in the morning. It is most commonly seen in middle-aged women, though it can also occur in younger male athletes.
In most cases, the condition improves with rehabilitation, insoles, and pain-relieving medication. However, a proportion of patients develop refractory plantar fasciitis that is difficult to treat, and some require extracorporeal shock wave therapy or surgery.
Q What are the symptoms of plantar fasciitis?
Many patients experience a sharp pain in the heel when first placing the foot on the floor upon waking in the morning. The pain typically originates slightly anterior to and on the inner side of the heel. It often eases as the foot is used during morning activity and may be forgotten entirely by the time morning preparations are complete. However, pain can return when standing up after sitting for a prolonged period, such as after sitting at a desk.
In the early stages, pain during exercise is relatively uncommon; it more typically intensifies after exercise.
Q What causes plantar fasciitis?
The plantar fascia acts like a bowstring stretched between the heel and the toes, absorbing impact with each step. When the fascia is subjected to excessive load — through running, weight gain, or other factors — small areas of damage can develop near the heel insertion. If these injuries heal promptly, no symptoms arise. However, as the body ages, healing becomes slower and incomplete.
When tissue damage occurs, the body responds by increasing blood vessel formation. Because blood vessels and nerve fibers grow together as a biological principle, abnormal vessels and nerves accumulate at the heel insertion of the plantar fascia. This renders the area hypersensitive and gives rise to sharp pain.
For those interested in learning more about these abnormal blood vessels, please also refer to
Risk factors for plantar fasciitis include:
- Age — the condition is most common between the ages of 40 and 60
- High-impact activities such as running, ballet dancing, and aerobics
- Flat feet or, conversely, high arches (excessively raised arch)
- Obesity
- Occupations that require prolonged standing on hard surfaces (such as factory work or teaching)
Q My heel has been painful for over six months. How long does plantar fasciitis take to heal?
Some patients recover spontaneously, but a proportion develop refractory plantar fasciitis that proves difficult to resolve. In refractory cases, pain can persist for more than a year, or even for several years. With appropriate treatment, improvement is achievable; however, cases in which inappropriate treatment is repeated without addressing the underlying cause are not uncommon, and many patients find themselves unable to recover despite ongoing efforts.
As described above, plantar fasciitis involves the proliferation of abnormal blood vessels alongside nerve fibers. Addressing this underlying mechanism leads to reliable improvement. For more details, please see the final section of this page.
Q Are there effective stretches for plantar fasciitis?
Maintaining flexibility in the plantar fascia itself helps reduce the stress placed on the insertion site when the fascia is stretched during activity. Massaging the sole of the foot can improve the flexibility of the plantar fascia. With the toes bent back (extended), massage the arch of the foot. Take care to avoid massaging directly over the painful heel area.
Stretching the gastrocnemius and soleus muscles (the calf muscles) can also help reduce the stress transmitted to the plantar fascia through the heel bone. To perform this stretch:
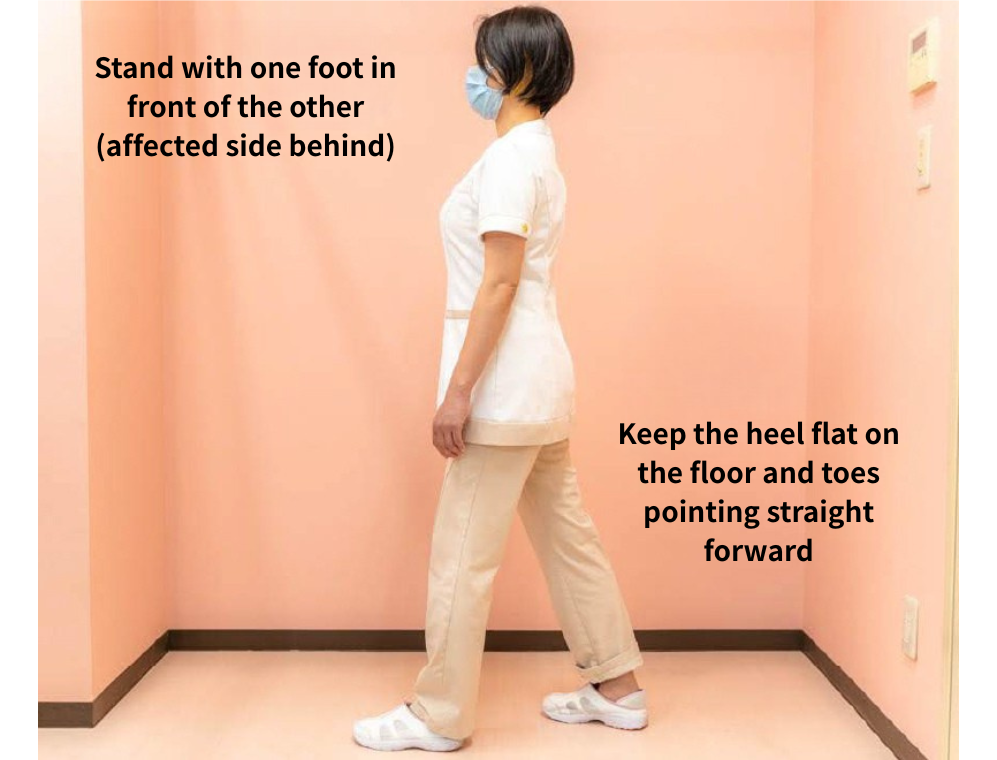
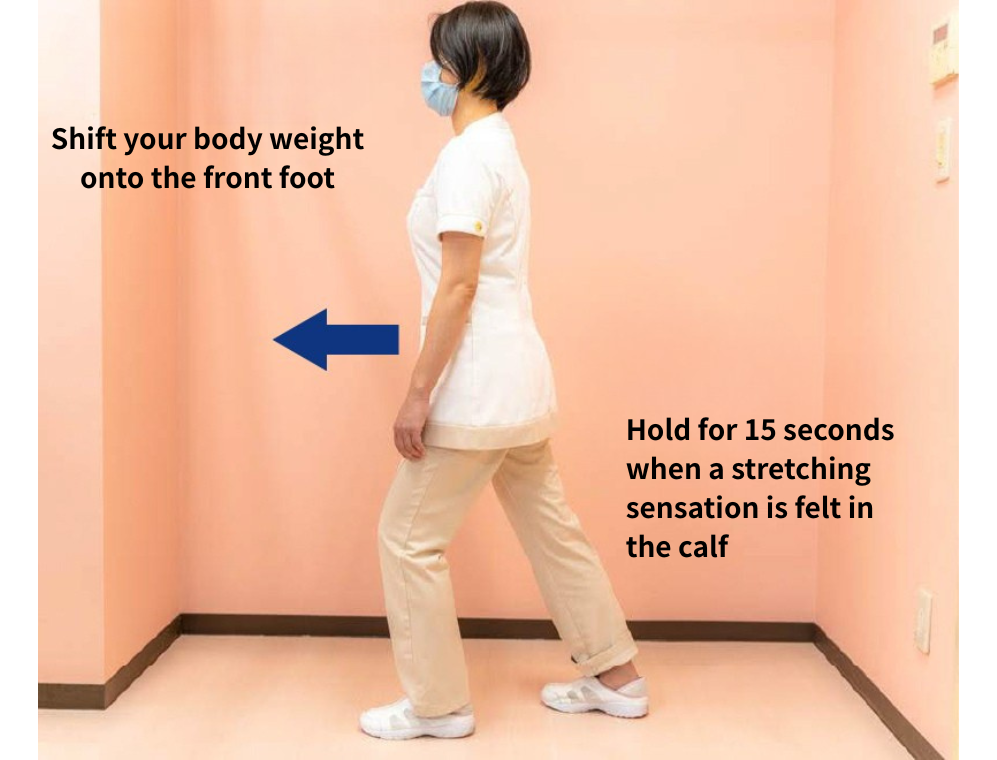
Stand with one foot in front of the other, with the affected foot placed behind. Keep the heel of the back foot flat on the floor with the toes pointing straight forward, and shift the body weight onto the front foot. A stretching sensation will be felt in part of the calf of the back leg. Hold this position for 15 seconds.
- Stand with one foot in front of the other, with the affected side behind. Keep the heel flat on the floor and the toes pointing straight forward.
- Shift the body weight onto the front foot. Hold when a stretching sensation is felt in the calf, for 15 seconds.
Q Is taping effective for plantar fasciitis?
The appropriate taping method depends on the individual's foot type.
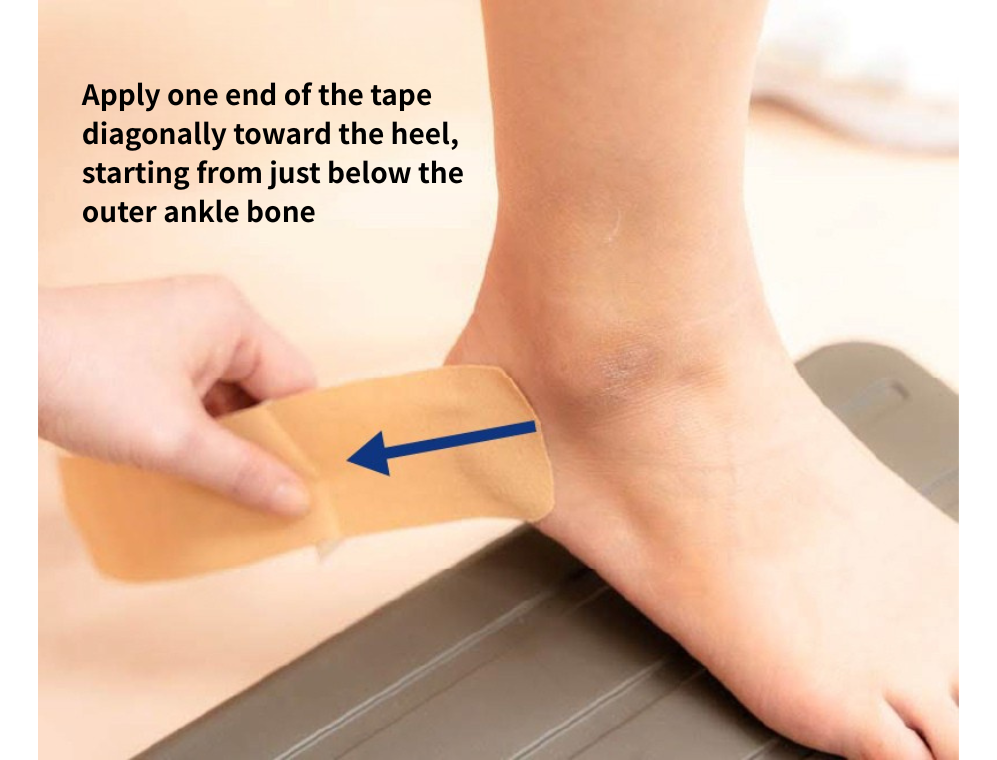
For patients with flat feet, taping that prevents the heel from rolling inward and raises the medial longitudinal arch (instep) is effective.
- Begin by applying one end of the tape diagonally toward the heel, starting from just below the outer ankle bone.
- Continue the tape around the heel and up past the inner ankle bone.
- Bring the tape across the front of the ankle and finish on the outer side of the shin.



For patients with high arches, taping that prevents the heel from rolling outward, or taping applied along the sole from the outer heel to the base of the big toe, is effective in reducing the stretch stress placed on the plantar fascia.
Q I have been advised to use insoles. What type of insole is effective for plantar fasciitis?
For patients with flat feet who experience pain on the heel side of the sole, insoles that raise the inner (big-toe) side of the heel to prevent inward rolling, or that elevate the medial longitudinal arch, are effective in reducing stress on the plantar fascia. Consultation with a specialized medical institution is recommended to determine the most appropriate option.
Q My doctor has recommended extracorporeal shock wave therapy (ESWT). How effective is it, and what are the risks?
A number of studies have examined the effectiveness of extracorporeal shock wave therapy for plantar fasciitis. While results vary across studies, the general consensus is that approximately 40% or more of patients achieve a reduction in pain to 50% or less of the original level. This means that complete pain relief cannot be guaranteed for all patients.
Serious complications from ESWT are rare. However, the treatment itself can be painful. Reported side effects include discomfort, pain, and bruising. In addition, because normal nerve fibers may be damaged by the shock waves, cases of bony deformity in the foot and plantar fascia rupture have also been reported. Patients who prefer to explore alternatives to shock wave therapy are encouraged to read the final section of this page.
Q What surgical options are available for plantar fasciitis?
Endoscopic surgery is available for plantar fasciitis, though it can only be performed at specialized medical institutions. Surgical options include plantar fascia release (partial excision of the plantar fascia) and heel spur removal (excision of the bony prominence). However, some reports indicate that success rates are not particularly high, and complete pain relief cannot be guaranteed.
Q I underwent ESWT but my pain has not improved and has actually worsened. Are there other effective treatments?
Extracorporeal shock wave therapy does not directly target the underlying cause of plantar fasciitis pain, which is why a proportion of patients do not respond to the treatment. As described earlier in this page, plantar fasciitis involves the co-proliferation of abnormal blood vessels and nerve fibers, which is a known driver of difficult-to-treat pain. When severe pain has persisted for several months or more, the presence of abnormal blood vessel proliferation is likely responsible for the treatment resistance.
A newer treatment designed to reduce these abnormal blood vessels is now available. The procedure takes only 5 to 10 minutes and has become increasingly accessible in recent years. For those who would like to learn more, please also refer to
Author

-
I began my career as an interventional radiologist, which led to my research on pathological angiogenesis during graduate school. As first author, I published findings on related genes in Nature Medicine in 2012. Based on this work, I developed a novel embolization treatment for chronic musculoskeletal disorders, such as knee osteoarthritis and frozen shoulder, and was the first to report its safety and effectiveness. This approach is now being studied internationally.
-Career-
2006-2009 Fellow, Department of Radiology, Clinica ET, Yokohama, Japan
2009-2012 Researcher, Center for Integrated Medical Research, Keio University, Tokyo, Japan
2012-2015 Clinical Researcher, Department of interventional radiology, Edogawa Hospital, Tokyo, Japan
2015-2017 Director, Musculoskeletal Intervention Center, Edogawa Hospital, Tokyo, Japan
2017- Chief Director, Okuno Clinic., Tokyo, Japan
Latest posts
 Jun 7, 2026Vocal Cord Inflammation (Chronic Laryngitis) FAQ
Jun 7, 2026Vocal Cord Inflammation (Chronic Laryngitis) FAQ Jun 7, 2026Interstitial Cystitis FAQ
Jun 7, 2026Interstitial Cystitis FAQ Jun 7, 2026Plantar Fasciitis FAQ
Jun 7, 2026Plantar Fasciitis FAQ Jun 5, 2026Achilles Tendinitis FAQ
Jun 5, 2026Achilles Tendinitis FAQ