Table of Contents
Q What is hip osteoarthritis?
Hip osteoarthritis is a condition in which the cartilage in the hip joint gradually wears away, causing the bone to deform and resulting in pain and reduced mobility in the groin area. It most commonly develops in people in their 40s and 50s, and is approximately four times more common in women than in men. It is estimated that 1.0–2.4% of the Japanese population — roughly 1.2 to 3 million people — have hip osteoarthritis.(1)
Approximately 80% of cases of hip osteoarthritis are caused by a condition known as acetabular dysplasia, which is described in detail below.
Because hip osteoarthritis progresses gradually over time, early and effective treatment is important to prevent worsening of the condition.
Women are more than four times more likely to develop hip osteoarthritis than men What is acetabular dysplasia — the leading cause of hip joint deformity and pain?
The three causes of acetabular dysplasia:
- Positioning and carrying methods during infancy
- Intense physical activity during middle school years
- Posterior pelvic tilt due to spinal curvature in older age
Q What causes hip osteoarthritis, and why is it more common in women?
The most common underlying cause of hip osteoarthritis in Japan is a structural problem known as acetabular dysplasia. This condition occurs overwhelmingly more often in women (89% of cases), which is why hip osteoarthritis as a whole is significantly more prevalent in women.(2)
In addition to acetabular dysplasia, other factors that increase the risk of developing hip osteoarthritis include obesity, genetic predisposition, and physically demanding occupations involving heavy lifting.(3) Rheumatoid arthritis and a history of hip injury or fracture may also contribute.
Q What is acetabular dysplasia, and what causes it?
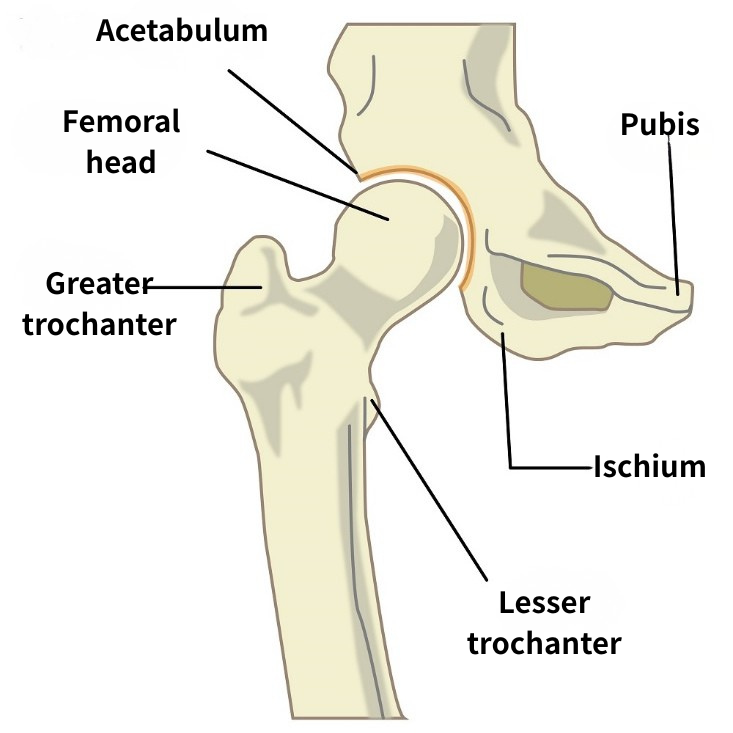
The hip joint consists of the femoral head — a ball-shaped structure — which fits into the acetabulum, a cup-shaped socket that acts as a roof over the ball. The broader and deeper the coverage provided by the acetabulum, the more stable the joint. Acetabular dysplasia is a condition in which the acetabulum does not develop to full size during growth, leaving the femoral head insufficiently covered. Symptoms are often absent in the teens and twenties, but mild pain may begin to emerge in the thirties and forties.
Although acetabular dysplasia is sometimes described as "something you are born with," it is not necessarily determined at birth. Genetic factors — such as naturally lax joints — play a role, but the condition is also known to develop as a result of the following three causes during postnatal growth:
I. Hip dislocation or subluxation in the newborn period (0–3 months), and delayed treatment
In newborns, inappropriate positioning during sleep, carrying methods, or the way diapers and clothing are applied can prevent the hips from remaining in an open position, leading to dislocation or subluxation of the hip joint. The natural position for a newborn's hips is one in which the legs are spread open; in this position, the hip joint is under minimal stress. However, if the legs are kept extended or the knees held together for extended periods, the risk of dislocation increases.
Hip dislocation of this type occurs more often on the left side (70% of cases) and is more common in girls. It is also most frequently seen in babies born in December and least often in those born in June — suggesting that the colder weather in the first three months after birth may lead to excessive bundling, which restricts hip movement. Carrying a baby in the koala position (upright, straddling the caregiver) reduces the risk of dislocation, whereas carrying in the horizontal position may prevent the hips from opening properly and can contribute to dislocation.
Furthermore, if hip dislocation goes undetected for too long, even after it is eventually treated, normal hip development may be compromised, leading to acetabular dysplasia later in life.
II. High-intensity sport during middle school years, particularly in girls
Acetabular dysplasia is not caused only by events in the newborn period. Around the ages of 12 and 13, the bones are in an active period of growth. Engaging in intense physical activity during this time — particularly in girls — can interfere with the development of the ilium, including the acetabulum. If the acetabulum stops growing while it is still small, acetabular dysplasia may result.
III. Posterior pelvic tilt in older age
As people age, a loss of muscle strength and stiffening of the spine can cause the pelvis to tilt backward. This can result in insufficient coverage of the front of the femoral head, leading to acetabular dysplasia.
A Japanese study examining 106 patients who progressed from acetabular dysplasia to hip osteoarthritis found that 43 cases were attributable to cause I., 33 to cause II., and 21 to cause III., with the remaining 9 cases not fitting any of the three categories.
Q What are the symptoms of hip osteoarthritis?
The symptoms of hip osteoarthritis most commonly appear during everyday movements. Pain in the front or outer side of the thigh may occur when tying shoelaces, rising from a chair, or beginning to walk. As the condition becomes more severe, pain may occur more frequently — including when turning over in bed at night or even at rest. Clicking or crunching sounds in the joint may also indicate advancing deformity.
Pain may also radiate to adjacent areas, including the knee and lower back.
Q How is hip osteoarthritis diagnosed, and what does an X-ray show?
Hip osteoarthritis is confirmed through X-ray examination, which allows assessment of the degree of cartilage wear and bone deformity. X-rays are also used for the stage classification described below and are useful for monitoring disease progression over time.
MRI provides more detailed information, including cartilage thinning, abnormalities in the bone marrow, the degree of fluid accumulation within the joint (edema), and the condition of the surrounding ligaments and muscles.
Q What are the stages of hip osteoarthritis?

Normal

Early stage

Advanced stage
Hip osteoarthritis is classified into the following stages of progression:
Stage 1: Pre-osteoarthritis Structural abnormalities of the hip joint are present, but the articular cartilage is still intact. Within 10 years of the onset of initial hip pain, approximately 30% of patients progress to the next stage.
Stage 2: Early osteoarthritis The articular cartilage begins to wear away and the joint space starts to narrow. On X-ray, increased density (sclerosis) may appear around the bone margins. At this stage, rehabilitation focused on strengthening the surrounding muscles is particularly important. Within five years, approximately 90% of patients tend to progress to the next stage.
Stage 3: Advanced osteoarthritis Widespread degeneration of the articular cartilage occurs and the joint space narrows significantly. Cysts may form within the bone, and bony spurs (osteophytes) may develop on the bone surface. Deformity is progressive, and joint replacement surgery begins to be considered more frequently. Squatting may become difficult due to reduced range of motion, and pain during joint movement and walking may increase.
Stage 4: End-stage osteoarthritis Cartilage loss is extensive and clear structural destruction of the joint is evident on imaging. Pain intensifies and walking may become restricted. At this stage, total hip replacement surgery is typically recommended.
Q How quickly does hip osteoarthritis progress?
Although acetabular dysplasia is the most common underlying cause of hip osteoarthritis, its presence does not mean that degeneration will progress rapidly. For many years, the condition may advance very slowly with minimal cartilage loss — but once degeneration begins, cartilage can deteriorate significantly over a period of approximately two years.
This is thought to occur because, up to a certain point, sufficient surrounding muscle strength and the protective effects of female hormones help maintain the structural integrity of the joint. A minor injury, menopause, or other trigger can then disrupt this balance, leading to a period of rapid inflammation and cartilage breakdown.
Q My X-ray did not look that bad, but I have significant pain in my groin. Why?
The degree of bone deformity seen on X-ray does not necessarily correspond to the intensity of hip pain. Some patients experience severe pain even when the X-ray shows relatively little deformity.
One reason for this is inflammation around the hip joint. Even when X-rays appear normal, an MRI may reveal fluid accumulation within the joint, indicating active inflammation — and this inflammation can be a significant source of pain.
It has also been found that areas of inflammation are frequently associated with abnormal blood vessel proliferation, and that nerves grow alongside these vessels — a combination that can give rise to pain that is difficult to resolve.
New treatments targeting these abnormal blood vessels are now available.
Q Can osteoarthritis affect just one hip, and can it cause a difference in leg length?
As described in the section on causes above, acetabular dysplasia — the most common underlying cause of hip osteoarthritis — can occur on one side only. In particular, dysplasia resulting from positioning or carrying methods during the newborn period is known to frequently affect only the left hip. It is therefore not uncommon for degeneration to develop on only one side in adulthood.
When osteoarthritis progresses on one side only, a discrepancy in leg length can develop. In advanced cases, a difference of approximately 1 to 3 cm between the two legs is possible.
Q I have been diagnosed with hip osteoarthritis. Are there activities I should avoid?
Activities that increase the daily load on the hip joint should be avoided. This is particularly important during the early to advanced stages, when active inflammation is present — movements that cause significant pain should be minimized as much as possible. Some patients push through pain in an effort to strengthen their muscles, for example by walking for long periods, but this places excessive strain on the hip joint and may accelerate disease progression.
At home, sitting on the floor should be avoided where possible; using chairs reduces the need to flex the hip deeply and lessens the load on the joint. Prolonged work in a low posture — such as mopping the floor or pulling weeds — should also be kept to a minimum.
In terms of exercise, dance, golf, and running place significant stress on the hip joint and should be avoided. Water walking is recommended, as it is gentle on the hip joint while still engaging the muscles effectively.
Q What does rehabilitation for hip osteoarthritis involve?
A physiotherapist will assess the patient's current level of pain, range of joint motion, and strength of the muscles surrounding the hip joint, as well as their gait, daily activities, and any sports or hobbies. An individualized rehabilitation plan is then developed based on the patient's specific goals.
Rehabilitation typically includes exercises to improve range of motion, strength training, balance exercises in sitting and standing positions, and practice of daily life and sports-related movements.
Q Are there effective stretches for hip osteoarthritis?
The hip joint moves in a variety of directions, but the movements most likely to become restricted in hip osteoarthritis are flexion and external rotation. Stretching in these directions can help improve the condition. Stretching the trunk is also important. The following stretches target each of these areas.
Flexion Stretch
Lie on the back. Bend one knee and hold it with both hands, drawing the knee toward the chest. Take care to keep the opposite leg flat on the floor. If strong pain is felt, do not force the movement — go only as far as is comfortable. If the stretch can be performed without pain, hold for 30 seconds with slow, steady breathing.


- Lie on the back.
- Bend one knee and hold it with both hands, drawing it toward the chest.
- A stretching sensation should be felt around the buttock (the area marked with a red circle). Hold for 30 seconds with slow, steady breathing.
Note: Take care to keep the opposite knee from lifting off the floor.
External Rotation Stretch
Lie on the back. Bend one knee to approximately 90 degrees and allow it to fall outward, going only as far as is comfortable and pain-free. Take care to keep the opposite hip from lifting off the floor. Hold for 30 seconds with slow, steady breathing.


- Lie on the back.
- Bend one knee to approximately 90 degrees and slowly lower it outward to one side.
- Hold within the available range for 30 seconds with slow, steady breathing.
Perform 3 sets on each side.
Note: Take care to keep the opposite hip from lifting off the floor.
Core (Trunk) Stretch
Sit on a chair and alternate between rounding and extending the back. When rounding the back, draw the navel inward and tilt the pelvis backward while leaning the upper body forward. When extending the back, push the navel forward to bring the pelvis upright and open the chest. Repeat within a comfortable range of motion.

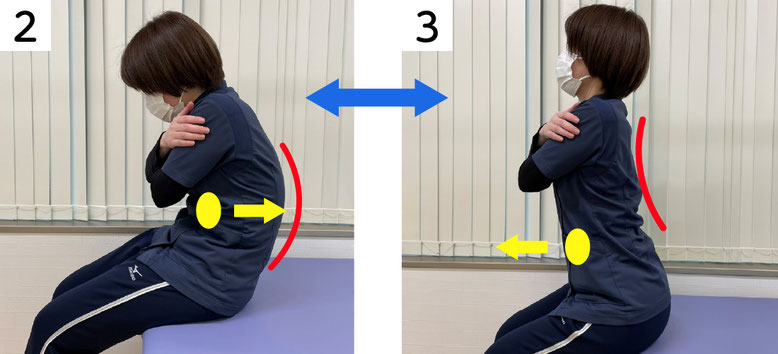
- Sit on a chair.
- Draw the navel backward and round the back.
- Push the navel forward and extend the back.
- Slowly repeat steps 2 and 3, 10 times.
Q What strength training exercises are effective for hip osteoarthritis?
In addition to stretching, strength training is recommended as a self-care measure for hip osteoarthritis. Exercises that engage the muscles controlling spinal movement are particularly beneficial. The following method is recommended.
Training Exercise
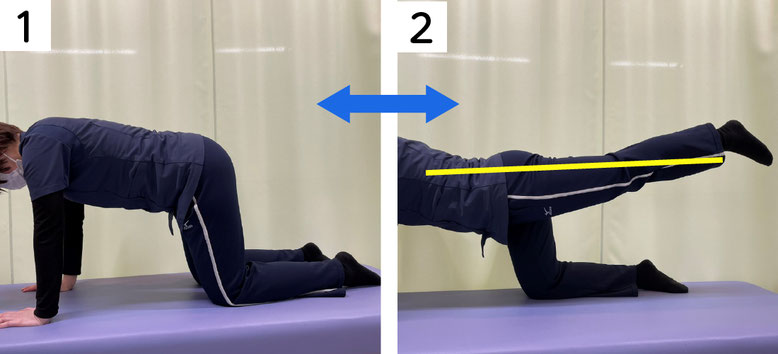
- Begin on all fours.
- Slowly lift one leg off the floor and extend it straight behind the body, keeping the knee straight so that the leg forms a straight line with the torso.
- Hold for approximately 5 seconds, then lower the leg and return to the starting position. Repeat with the opposite leg, also holding for 5 seconds.
- Perform 10 repetitions on each side.
Note: Do not perform this exercise on a hard floor, as it may cause pain in the kneecap. Use a mat or futon for cushioning.
Q Should rehabilitation and exercise therapy be continued even when painful?
If pain persists until the following day after rehabilitation or exercise, the intensity is too high and should be reduced or temporarily stopped. Walking and jogging place significant stress on the hip joint and are not suitable as exercise therapy. These activities should be replaced with lower-impact alternatives such as water walking or swimming, which are gentler on the hip joint.
Q What non-surgical treatments are available for hip osteoarthritis?
While there is no treatment that can reverse structural bone deformity in hip osteoarthritis, several options are available to help relieve pain and improve mobility.
Conservative (non-surgical) treatments include:
- Lifestyle modification and weight loss
- Physical therapy
- Assistive devices (canes, walkers, etc.)
- Medications (loxoprofen, acetaminophen, tramadol, etc.)
- Injection therapy (hyaluronic acid, steroids, etc.)
More recently, a newer conservative treatment has also become available: catheter-based therapy, which is used to reduce the abnormal blood vessels that form around the hip joint.
Q What surgical options are available for hip osteoarthritis?
Surgery may be recommended when conservative treatment does not provide sufficient improvement.
Hip Resurfacing: The damaged bone and cartilage of the acetabulum (hip socket) are removed and replaced with a metal shell. The femoral head itself is preserved and covered with a smooth metal cap.
Total Hip Replacement (THR): Both the damaged acetabulum and the femoral head are removed and replaced with new joint surfaces made of metal, plastic, or ceramic, restoring hip function.
The timeline for returning to work and the course of rehabilitation following hip surgery depend on the type of procedure performed. Physical therapy is commonly used to restore strength and range of motion. Crutches or a mobility aid may be required for a period after surgery. It is recommended that patients discuss the details of postoperative recovery directly with their treating physician.
References
(1) Inoue K, Wicart P, Kawasaki T et al: Prevalence of hip osteoarthritis and acetabular dysplasia in French and Japanese adults. Rheumatology (Oxford) 2000; 39(7): 745–8
(2) Hattori T, Inaba Y, Ichinose S, et al. The epidemiology of developmental dysplasia of the hip in Japan: Findings from a nationwide multi-center survey. J Orthop Sci 2017; 22: 121–6
(3) Yoshimura M, Sasaki S, Iwasaki K et al: Occupational lifting is associated with hip osteoarthritis: a Japanese case-control study. J Rheumatol 2000; 27(2): 434–40
Author

-
I began my career as an interventional radiologist, which led to my research on pathological angiogenesis during graduate school. As first author, I published findings on related genes in Nature Medicine in 2012. Based on this work, I developed a novel embolization treatment for chronic musculoskeletal disorders, such as knee osteoarthritis and frozen shoulder, and was the first to report its safety and effectiveness. This approach is now being studied internationally.
-Career-
2006-2009 Fellow, Department of Radiology, Clinica ET, Yokohama, Japan
2009-2012 Researcher, Center for Integrated Medical Research, Keio University, Tokyo, Japan
2012-2015 Clinical Researcher, Department of interventional radiology, Edogawa Hospital, Tokyo, Japan
2015-2017 Director, Musculoskeletal Intervention Center, Edogawa Hospital, Tokyo, Japan
2017- Chief Director, Okuno Clinic., Tokyo, Japan
Latest posts
 Jun 7, 2026Vocal Cord Inflammation (Chronic Laryngitis) FAQ
Jun 7, 2026Vocal Cord Inflammation (Chronic Laryngitis) FAQ Jun 7, 2026Interstitial Cystitis FAQ
Jun 7, 2026Interstitial Cystitis FAQ Jun 7, 2026Plantar Fasciitis FAQ
Jun 7, 2026Plantar Fasciitis FAQ Jun 5, 2026Achilles Tendinitis FAQ
Jun 5, 2026Achilles Tendinitis FAQ