Table of Contents
Q What is jumper's knee?
Jumper's knee, also known as patellar tendinitis, is a condition in which the patellar tendon — located just below the kneecap — becomes hypersensitive, causing pain during a wide range of activities including sports and daily life. It is commonly seen in people who perform repetitive jumping movements, such as volleyball, basketball, high jump, and soccer goalkeepers, as well as in runners.
Although the name includes the word "jumper," the condition is not limited to those who participate in jumping sports. It can also develop in long-distance runners such as marathon athletes, as well as in baseball players and athletes in other disciplines.
In some cases, jumper's knee resolves on its own without specific treatment. However, it is not uncommon for the condition to persist for a prolonged period without improvement. Patients whose symptoms do not resolve readily are advised to seek evaluation at a specialized medical institution.
Q Where does jumper's knee hurt, and what are the symptoms?
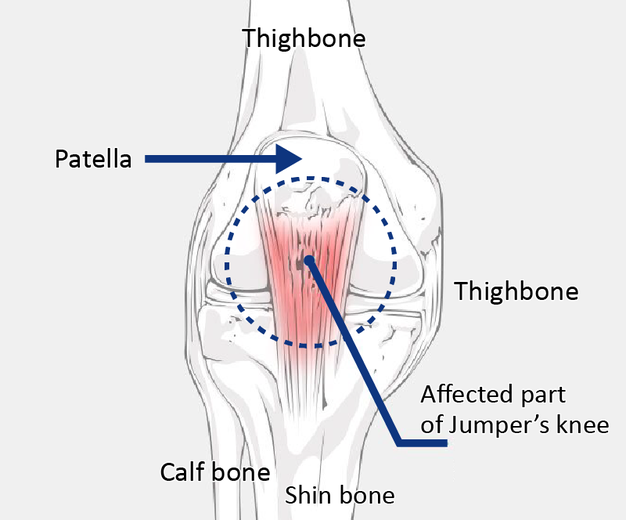
The formal medical term for jumper's knee is patellar tendinitis. The patellar tendon is located just below the kneecap — the area that makes direct contact with the ground when kneeling.
Characteristic symptoms include pain when climbing or descending stairs, pain during jumping, and pain while running.
Q What causes jumper's knee?
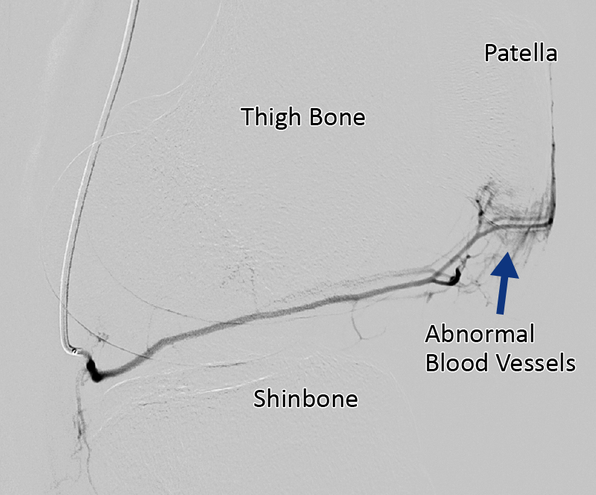
The underlying cause of jumper's knee (patellar tendinitis) is believed to be the abnormal proliferation of blood vessels within the patellar tendon, driven by repetitive strain.
Each time a jumping or landing movement is performed, the patellar tendon is placed under tension. When the strain is particularly strong, small tears can occur within the tendon. In response, new blood vessels form to facilitate healing. Under normal circumstances, these tears heal within approximately two weeks, after which the newly formed vessels recede. However, when strenuous activity continues before healing is complete, new damage occurs before the previous injury has resolved — and the blood vessels have no opportunity to diminish, leading to ongoing proliferation.
As blood vessels increase, nerve fibers grow alongside them, and this is what gives rise to pain. For more information about these abnormal blood vessels, please also refer to
Q How is jumper's knee diagnosed?
Diagnosis begins with a medical history, including questions about whether pain occurs during jumping, sprinting, or stair climbing. A physical examination is then performed to check for tenderness (pain on pressure) directly below the kneecap. Tenderness in this location both when the knee is extended and when it is bent is a strong indicator of jumper's knee.
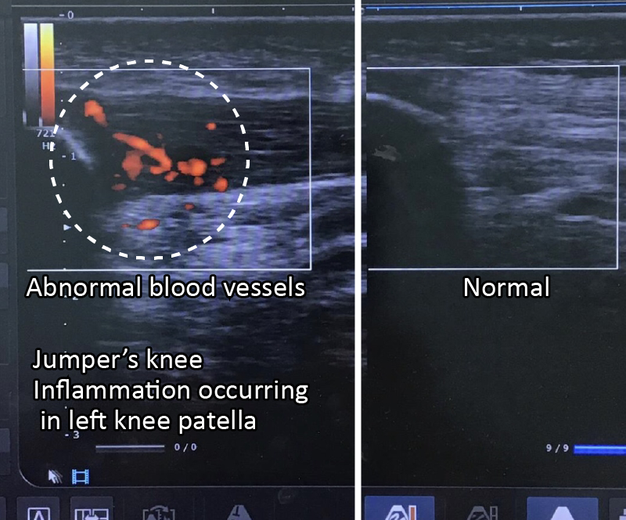
The diagnosis is confirmed through imaging. Ultrasound examination is commonly used, as it is quick and straightforward to perform.
The image below shows an actual ultrasound examination. Compared to the image on the right (normal), the image on the left (jumper's knee) shows a darkened, swollen tendon with red vascular signals invading the swollen tissue. MRI may also be used to confirm the diagnosis.
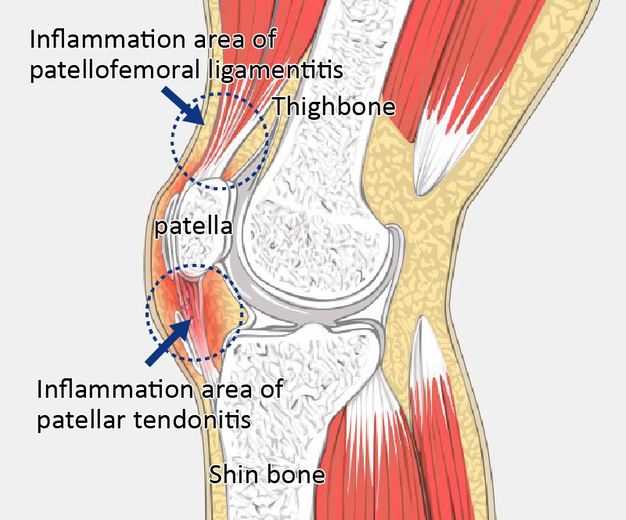
Q I have pain above the kneecap. Is this also jumper's knee?
Pain above the kneecap is most likely caused by a condition formally known as patellofemoral ligamentitis. However, this condition is also commonly grouped under the umbrella term "jumper's knee."
The treatment approach for patellofemoral ligamentitis is largely the same as for other forms of jumper's knee. Patients who are concerned about their symptoms are encouraged to consult a specialist.
Q Are injections effective for jumper's knee?
The effectiveness of injections for jumper's knee depends on the type of medication used.
Steroid injections have a strong anti-inflammatory effect but are not recommended for jumper's knee. Injecting steroids into a tendon such as the patellar tendon can weaken the tissue, and in the worst cases may lead to tendon rupture.
Hyaluronic acid injections do not carry the same risk of tendon weakening, but their effectiveness for this condition is limited. In general, injections should not be pursued without careful consideration. Consultation with a pain specialist is strongly advised before proceeding with any injection therapy.
Q Are there effective stretches for jumper's knee?
The following stretches are recommended for jumper's knee. For those who experience pain after training, performing these stretches immediately afterward as a cool-down routine is particularly effective.
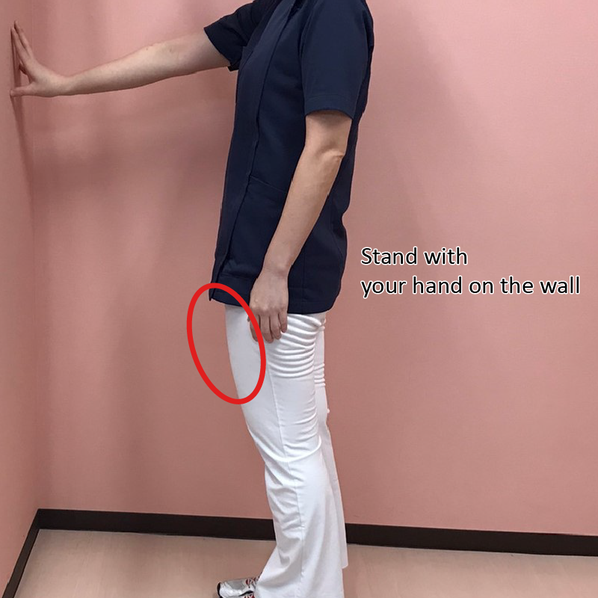
Stretch 1: Quadriceps stretch
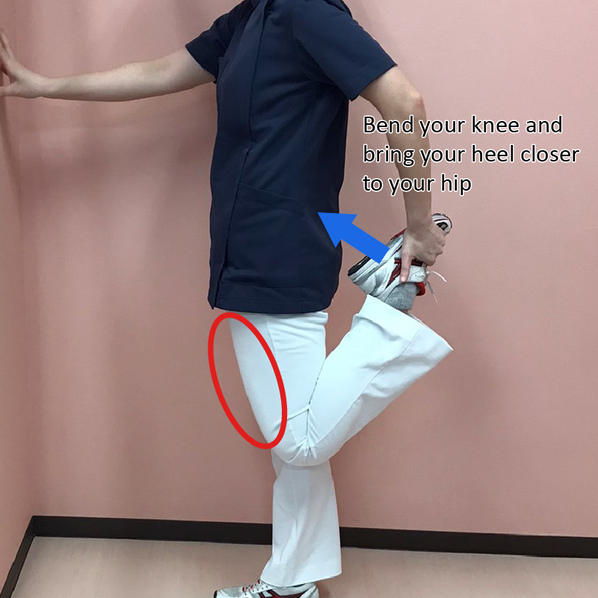
This stretch is performed standing on one leg. Using a desk or wall for support makes it easier to maintain balance.
- Stand and place one hand on a wall or desk for support.
- Bend the knee to be stretched, bringing the heel toward the buttock, and hold the top of the foot with the hand on the same side.
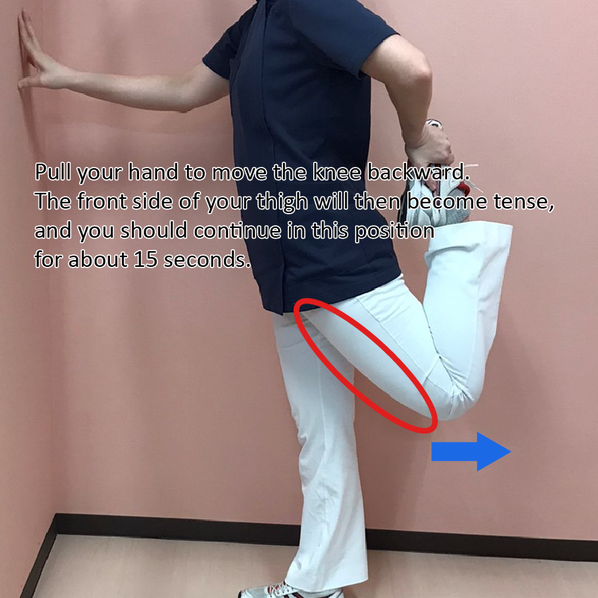
- While keeping the heel close to the buttock, draw the knee backward. A stretching sensation will be felt along the front of the thigh. Hold for 15 seconds.
Stretch 2: Iliopsoas stretch
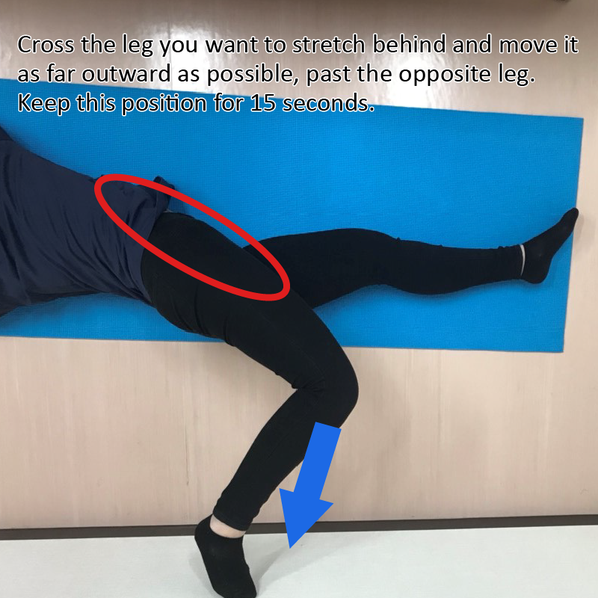
This stretch is performed lying face down with the arms extended overhead.
- Lie face down with both arms extended overhead.
- Cross the leg to be stretched behind the body, moving it as far outward as possible past the opposite leg. Keep the arm on the same side extended as far forward as possible.
- A stretching sensation will be felt in the iliopsoas muscle, located on the front (abdominal) side of the trunk and hip joint. Hold for 15 seconds.

Additional stretches targeting the quadriceps and iliopsoas muscles beyond those described here can also be beneficial. However, if pain is present not only after training but also during daily activities, stretching alone is unlikely to be sufficient. In such cases, evaluation at a specialized medical institution is recommended.
Q How can jumper's knee be prevented?
The stretches described above are also effective as preventive measures.
Since overuse is one of the contributing causes of jumper's knee, reducing training volume is necessary if pain develops after practice. In severe cases, jumper's knee can become a career-threatening injury. Rather than pushing through pain, patients are encouraged to seek evaluation from a specialist if symptoms are significant, so that an appropriate treatment plan can be established.
Q Are there effective taping or support braces for jumper's knee?
A band-style support brace that wraps around the knee just below the kneecap is available and is considered to offer some benefit in relieving symptoms of jumper's knee. However, if the pain is significant, continuing to train while relying on a brace to mask the discomfort risks worsening the condition and delaying return to sport. While taping around the knee is sometimes recommended, using it as a means to push through pain is not advisable.
If the condition does not seem to be improving, evaluation at a specialized medical institution is recommended.
Q It has been six months since I developed jumper's knee. Is there a way to speed up recovery?
In mild cases, jumper's knee may resolve within a few weeks. However, in more severe cases, recovery is not straightforward.
If symptoms are not improving despite rest and treatment, it is possible that the current treatment is not adequately targeting the underlying cause of the pain. As described above, the cause of pain in jumper's knee is the abnormal blood vessels and the nerve fibers that proliferate alongside them.
Unless the treatment directly addresses this underlying cause, the pain will not resolve. After six months of symptoms, the condition is likely to be severe. Consultation with a specialized medical institution is strongly recommended.
Normal Knee
Jumper’s Knee
Q Rehabilitation and injections have not improved my jumper's knee. Should I consider surgery, and what other treatments are available?
For severe cases that do not respond adequately to injections, catheter-based therapy is available. This treatment targets the abnormal blood vessels that are the underlying cause of jumper's knee pain, with the goal of achieving full recovery. For more details, please refer to the article:
Surgery is also an option, but it involves partial resection of the affected tendon — removing the original tissue and replacing it with tissue from another site. Surgical outcomes for this condition are generally not favorable, and residual pain or discomfort after surgery is not uncommon. Hospitalization is also required. For these reasons, surgery is not strongly recommended.
Author

-
I began my career as an interventional radiologist, which led to my research on pathological angiogenesis during graduate school. As first author, I published findings on related genes in Nature Medicine in 2012. Based on this work, I developed a novel embolization treatment for chronic musculoskeletal disorders, such as knee osteoarthritis and frozen shoulder, and was the first to report its safety and effectiveness. This approach is now being studied internationally.
-Career-
2006-2009 Fellow, Department of Radiology, Clinica ET, Yokohama, Japan
2009-2012 Researcher, Center for Integrated Medical Research, Keio University, Tokyo, Japan
2012-2015 Clinical Researcher, Department of interventional radiology, Edogawa Hospital, Tokyo, Japan
2015-2017 Director, Musculoskeletal Intervention Center, Edogawa Hospital, Tokyo, Japan
2017- Chief Director, Okuno Clinic., Tokyo, Japan
Latest posts
 Jun 7, 2026Vocal Cord Inflammation (Chronic Laryngitis) FAQ
Jun 7, 2026Vocal Cord Inflammation (Chronic Laryngitis) FAQ Jun 7, 2026Interstitial Cystitis FAQ
Jun 7, 2026Interstitial Cystitis FAQ Jun 7, 2026Plantar Fasciitis FAQ
Jun 7, 2026Plantar Fasciitis FAQ Jun 5, 2026Achilles Tendinitis FAQ
Jun 5, 2026Achilles Tendinitis FAQ