Table of Contents
Q What is golfer’s elbow?
Golfer’s elbow, formally known as medial epicondylitis, is a condition in which pain and inflammation develop in the tendons on the inner side of the elbow. It is characterized by pain along the inner aspect of the elbow extending toward the forearm and wrist.
Although it is called “golfer’s elbow,” the condition is not caused only by golf. It can also result from activities such as tennis forehand strokes, baseball throwing, carrying heavy trays or objects, hammering, or prolonged computer typing. In some cases, it may occur even without a clear history of excessive strain.
Golfer’s elbow is more common in women than in men and tends to occur more frequently in middle-aged adults, particularly those in their 40s and 50s.
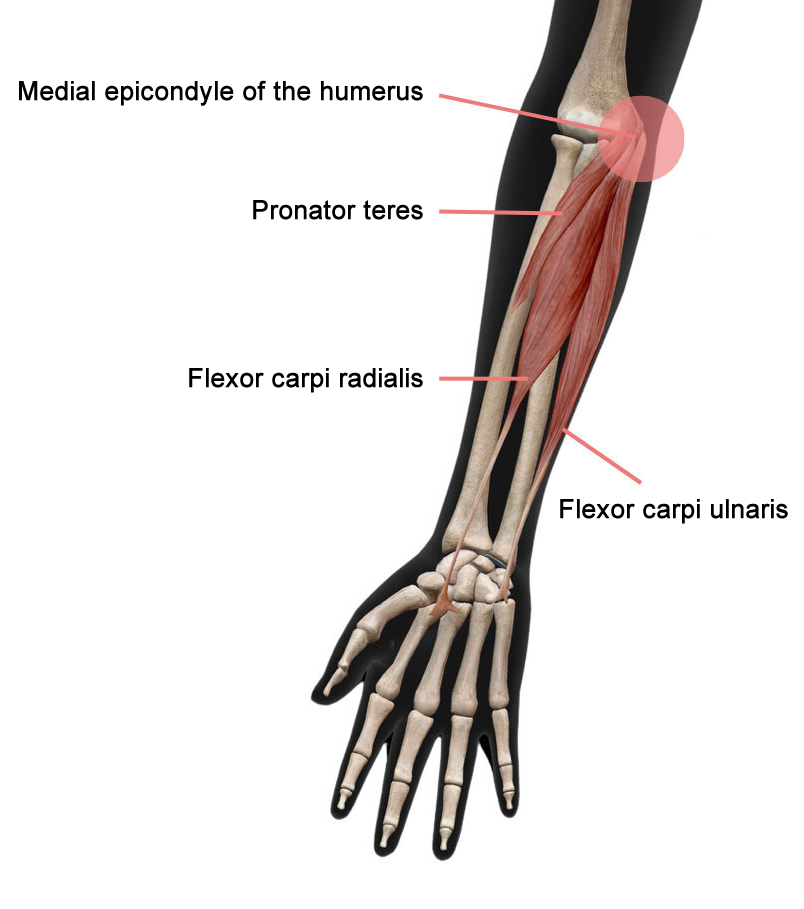
The pain is caused by damage or inflammation of the tendons of the pronator teres and the wrist flexor muscles (including the flexor carpi radialis and flexor carpi ulnaris) that attach to the inner part of the elbow (the medial epicondyle of the humerus).
What is the difference between tennis elbow and golfer’s elbow?
There is a condition called tennis elbow (lateral epicondylitis), which causes pain on the outer side of the elbow. Tennis elbow is more common than golfer’s elbow and is reported to occur 7 to 10 times more frequently.
The name of the condition is not determined by the sport that caused it. Even if the pain results from excessive golf activity, it is diagnosed as tennis elbow if the pain and inflammation are on the outer side of the elbow. Likewise, pain caused by playing tennis is diagnosed as golfer’s elbow if the pain and inflammation are on the inner side of the elbow.
What are the symptoms of golfer’s elbow?
Pain is felt when pressure is applied to the inner side of the elbow. The pain often extends to the forearm and wrist. Pain may occur when lifting objects such as bags, gripping items, twisting the wrist, or bending and straightening the elbow.
Daily activities such as carrying trays, pulling ropes, washing the face, or opening doors may also trigger pain. In some cases, stiffness may be noticed in the morning or after prolonged periods without elbow movement. Limited range of motion, such as difficulty fully extending or bending the elbow, may also occur.
What causes golfer’s elbow?
Golfer’s elbow is caused by repetitive movements or prolonged overuse that place stress on the inner side of the elbow. It commonly occurs during sports such as golf, tennis, or baseball, particularly when performing movements like those described below.
- When swinging a golf club, particularly just before the club makes contact with the ball or the ground, and at the moment of impact
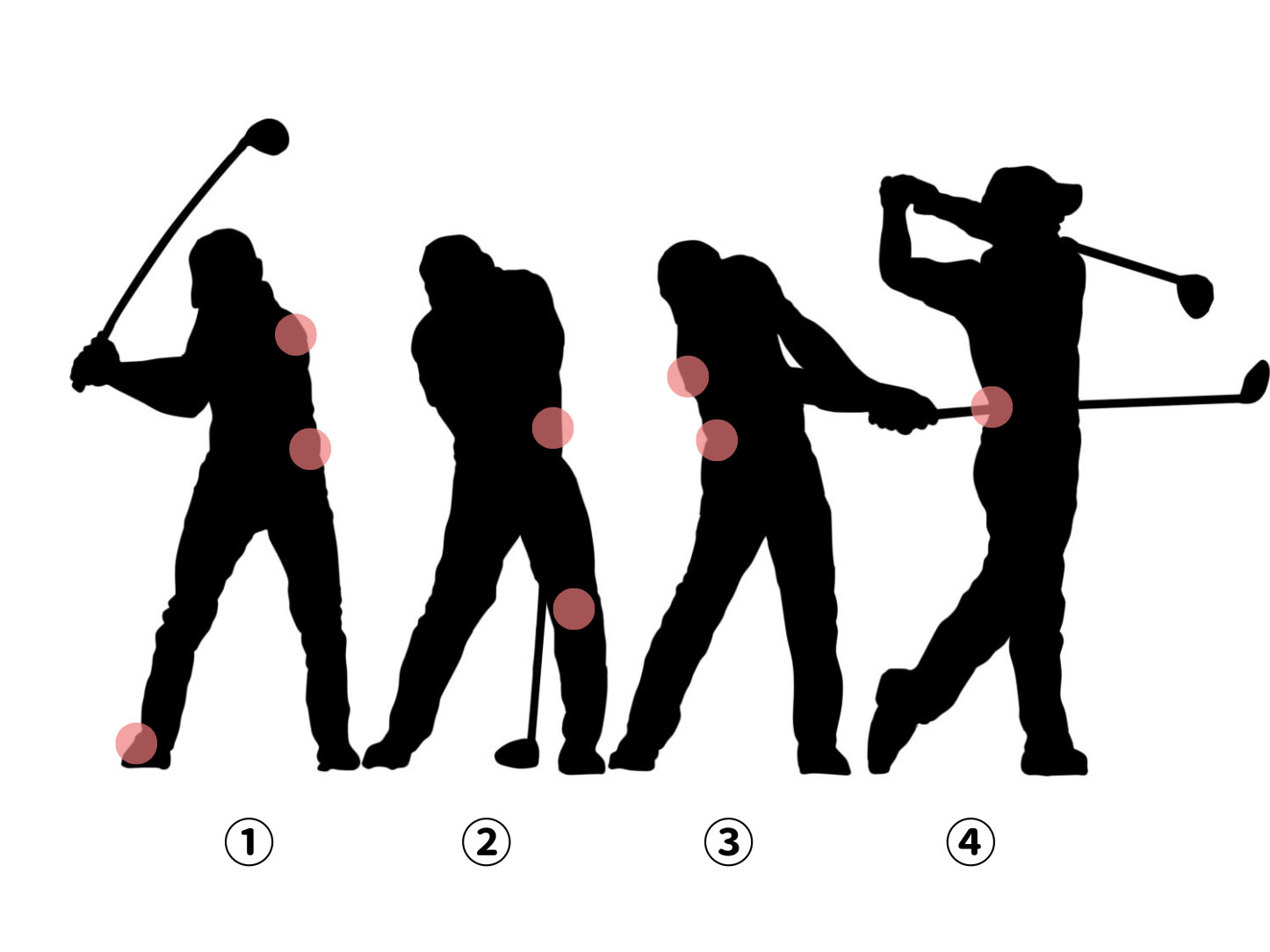
Areas that are prone to increased stress during a golf swing
- When performing a forehand stroke with a tennis racket.
- In baseball pitching, stress is applied to the elbow during ① the late cocking phase and ② the acceleration phase.
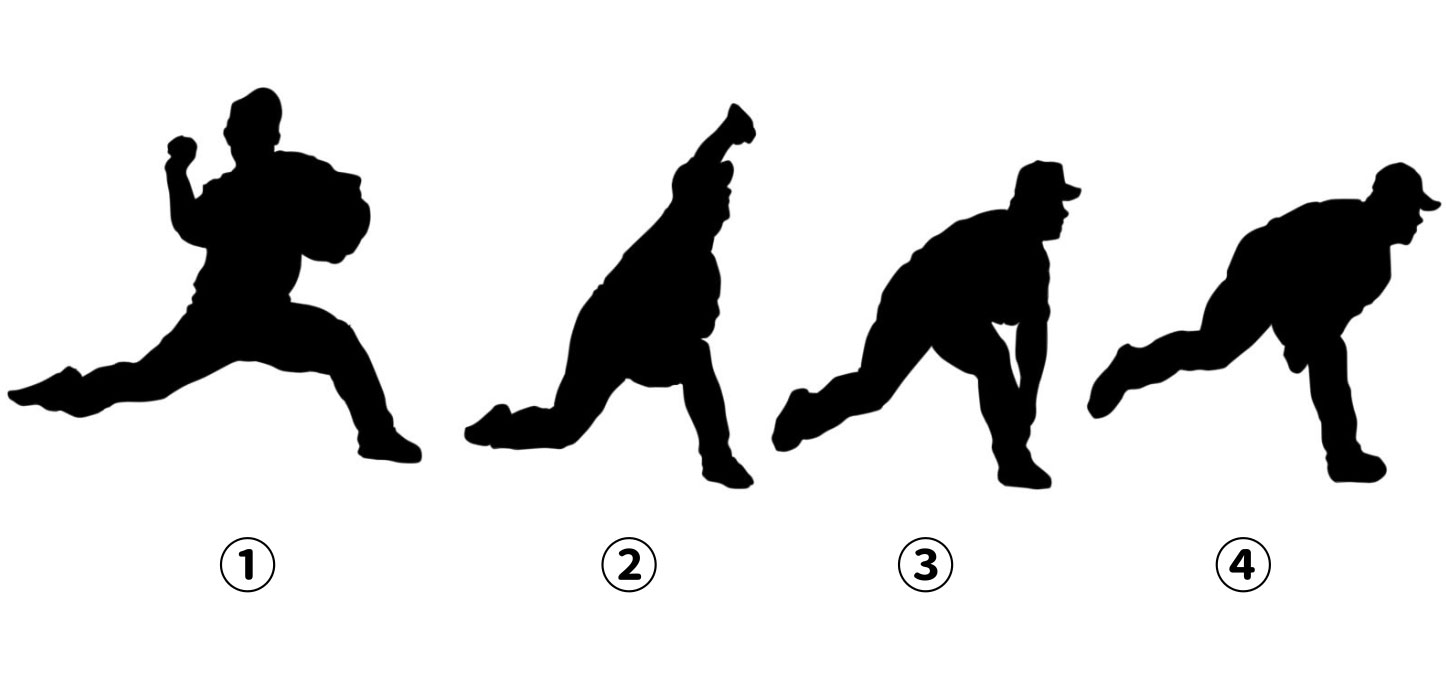
The baseball pitching motion
In addition to the three sports mentioned above, golfer’s elbow can also occur in athletes who participate in bowling, rock climbing, archery, and weightlifting.
It is also common among beginners who have improper sports techniques. It may occur when warm-up exercises before activity are insufficient, or when the muscles of the shoulder or wrist are weak.
Golfer’s elbow is not limited to athletes. It can also be seen in people whose daily activities or occupations involve lifting objects or throwing or swinging movements with the arm, such as carpenters, butchers, or catering staff.
In addition to these activity-related causes, smoking and diabetes may also be risk factors.
Risk factors
- Spending more than two hours per day performing repetitive movements
- Smoking
- Obesity
What tests are used to diagnose golfer’s elbow?
The diagnosis of golfer’s elbow can be made based on the patient’s medical history and physical examinations, including the following provocative tests.
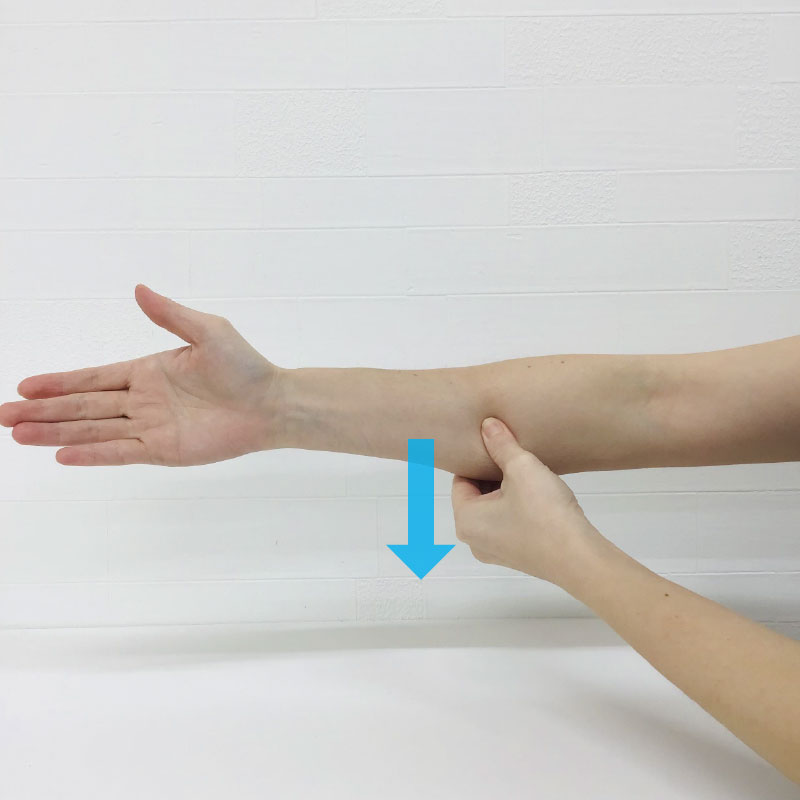
Physical examination (provocative test)

Place the painful elbow on a table with the palm facing upward.
With the physician applying downward pressure on the hand, the patient is instructed to extend the wrist. In cases of golfer’s elbow, this maneuver elicits pain on the medial side of the elbow.
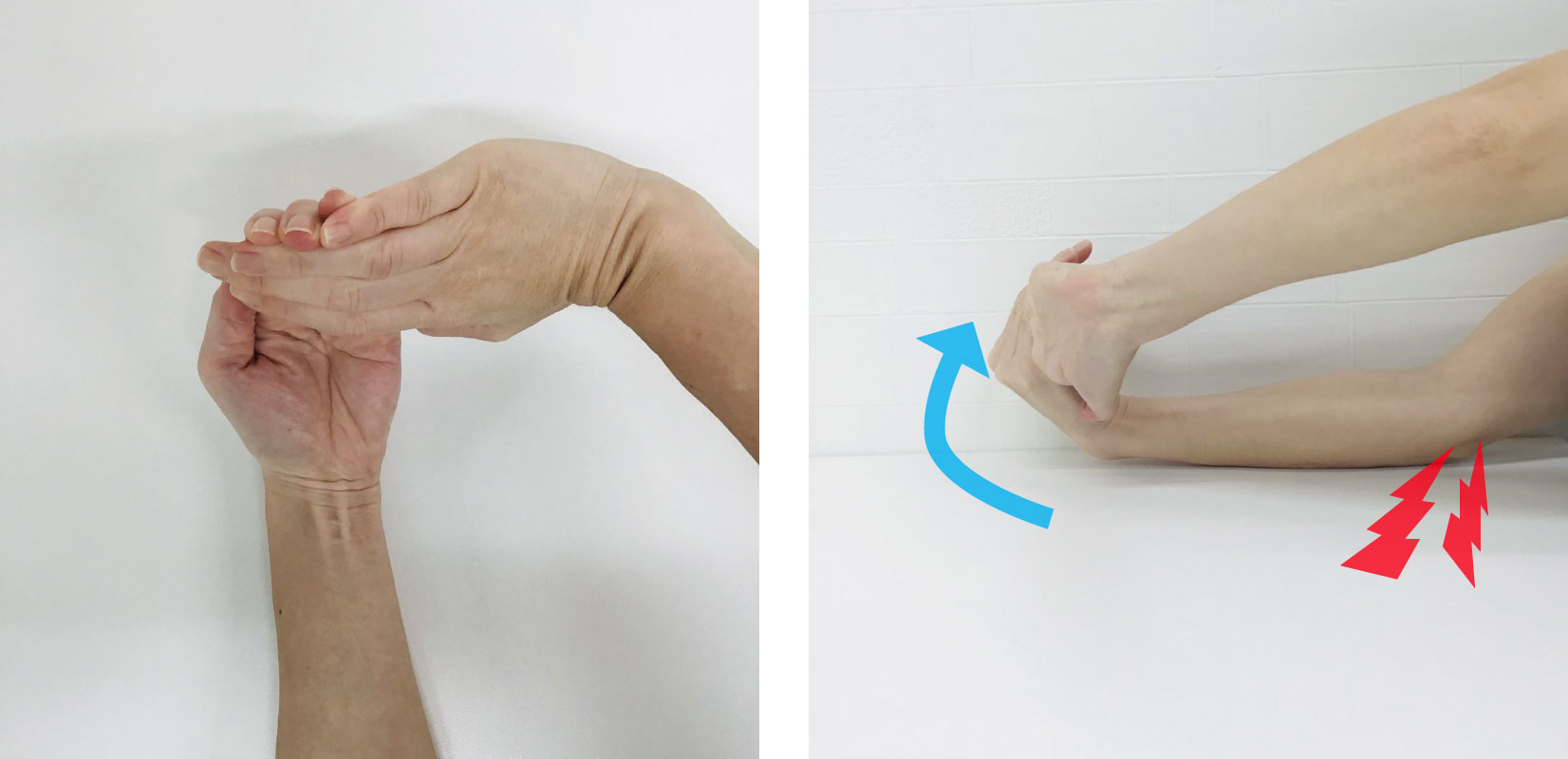
While the physician applies downward pressure on the hand from above, the patient is instructed to lift the hand from the wrist.
If conditions other than golfer’s elbow are suspected, the following examinations may be performed for differential diagnosis. Among these, magnetic resonance imaging (MRI) and ultrasonography (ultrasound examination) are considered the most effective.

MRI image showing golfer’s elbow, indicated by the white area marked with an arrow.
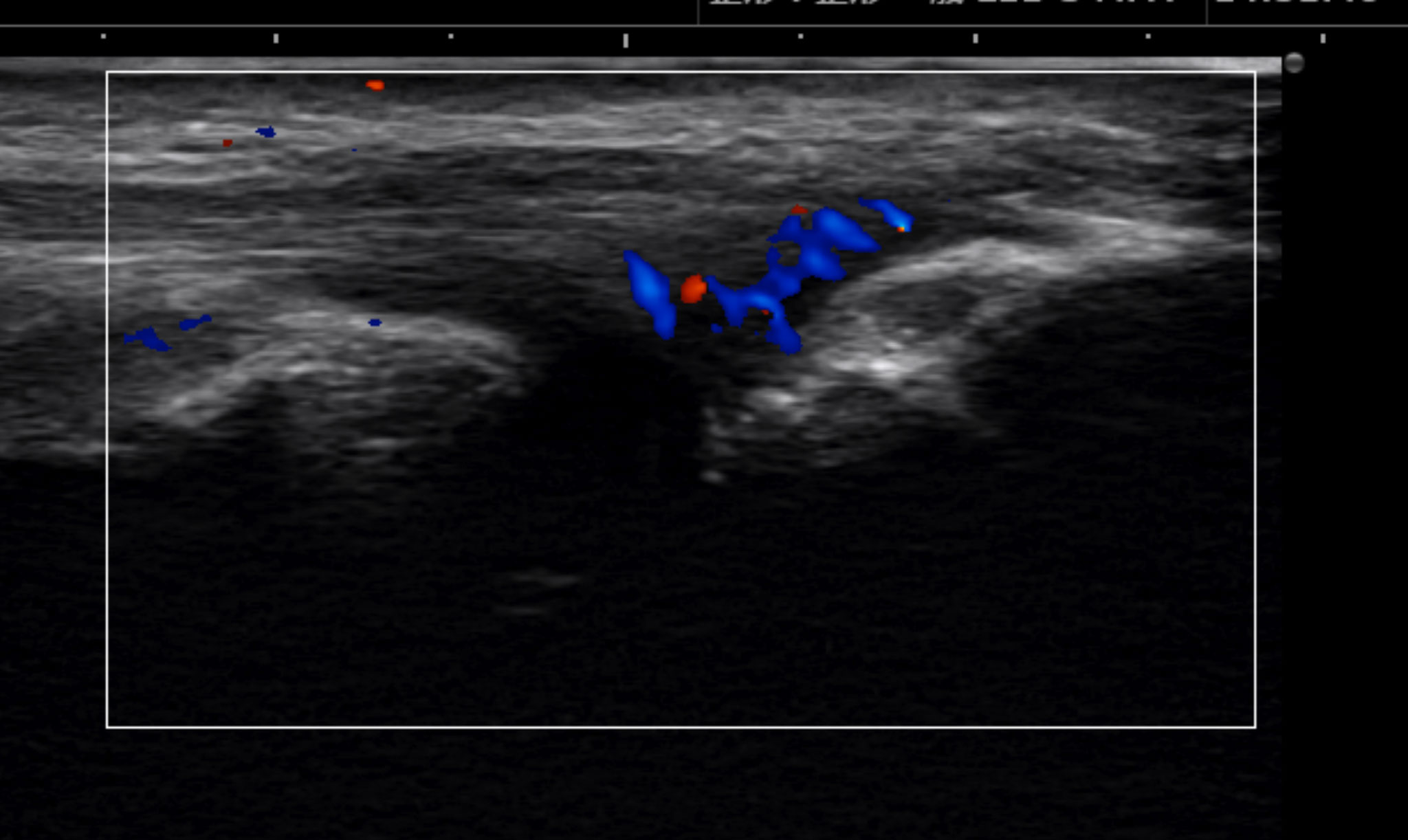
Ultrasound image: the red and blue areas indicate the site of pain.
Q How is golfer’s elbow treated?
Treatment options for golfer’s elbow
Initial treatment
For golfer’s elbow, it is important to rest the affected arm and avoid movements that cause pain. We recommend a period of rest for approximately six weeks. In addition to rest, most patients experience symptom improvement with the following conservative treatments:
- Applying ice to the affected area
- Using pain-relieving medications (anti-inflammatory drugs, NSAIDs, acetaminophen, etc.)
- Reducing stress on the elbow by using braces (elbow straps) or kinesiology tape
- Undergoing physical therapy (rehabilitation)
Additional treatment
If initial treatment does not provide sufficient relief, the following additional treatments may be effective:
Steroid injections
The number of steroid injections should be limited. We recommend no more than one, or at most two injections. Although steroid injections have a strong anti-inflammatory effect, they may also cause damage to the injected tissue. Repeated injections over time may increase tendon damage and lead to tendon weakening.
Platelet-rich plasma (PRP) injection
Using ultrasound guidance, platelet-rich plasma (PRP), prepared by centrifugation, is injected into and around the damaged tendon tissue.
Surgery
Surgery is performed only when symptoms do not respond to treatment after 6 to 12 months, or when there is significant tearing of the muscles or tendons. During surgery, damaged tissue is removed, and the tendon is repaired if necessary.
More recently, a new treatment option for refractory golfer’s elbow has become available: catheter-based therapy, which is performed as a day procedure and takes approximately 20 minutes. For those who would like to learn more, please refer to the treatment case examples provided here.
What self-care measures are recommended to help return to work and sports after treatment?
After treatment, once the pain has completely resolved, stretching exercises and isometric exercises are initiated. As recovery progresses further, resistance exercises are added, with the goal of improving muscle strength beyond the level prior to the onset of golfer’s elbow. When repetitive movements can be performed without discomfort, patients may return to sports or work.
Thereafter, a maintenance program is recommended to reduce the risk of recurrence and to maintain flexibility and muscle strength.
**Isometric exercises are a type of exercise involving static muscle contraction without visible joint movement.
What can be done to prevent golfer’s elbow?
To prevent golfer’s elbow, it is important to stretch and strengthen the muscles around the elbow, perform proper warm-up exercises before activity, and allow adequate rest time.
What stretches and massage techniques are effective for self-treatment of golfer’s elbow?
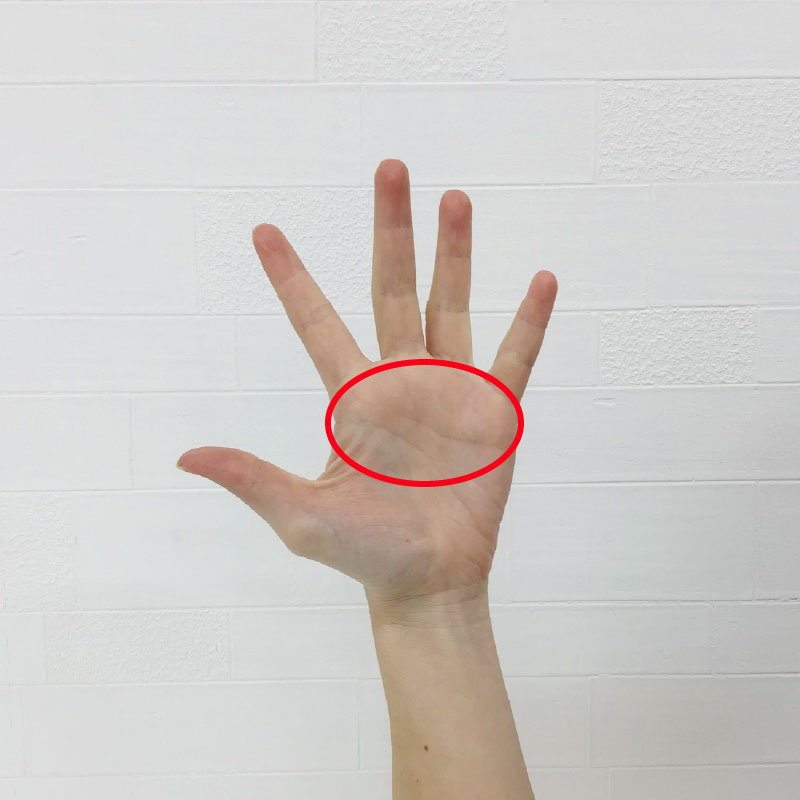
Palm stretching
When using the hands and fingers, if the palm (the area marked with a red circle) is tight, the finger muscles tend to be overused. This increases the load on the finger flexor muscles. Because the finger flexor muscles attach to the inner (medial) side of the elbow, excessive stress on these muscles can lead to pain on the medial side of the elbow. To reduce the load on the finger flexor muscles, palm stretching is recommended.
1.Bend the first and second joints of the four fingers—from the index finger to the little finger—on the affected side.
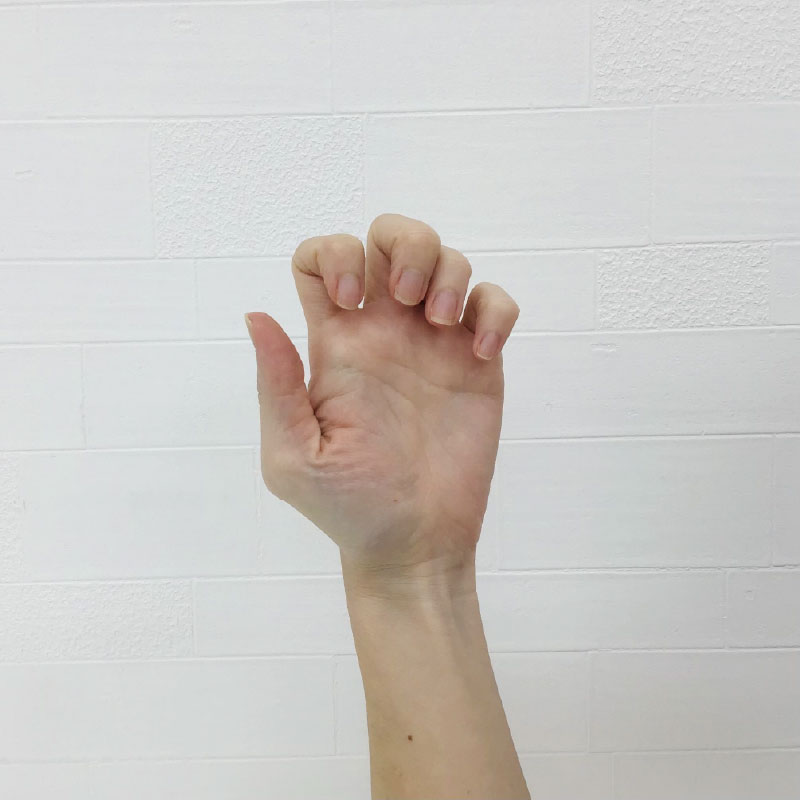
2.Use the fingertips of the opposite hand to grasp the fingers on the affected side, placing them against the bases of the fingers on the back of the hand (the area marked with a red

3.Slowly extend the fingers backward.

Lateral view photograph

Photograph viewed from the palm side. A stretching sensation is felt in the area marked with a red circle.
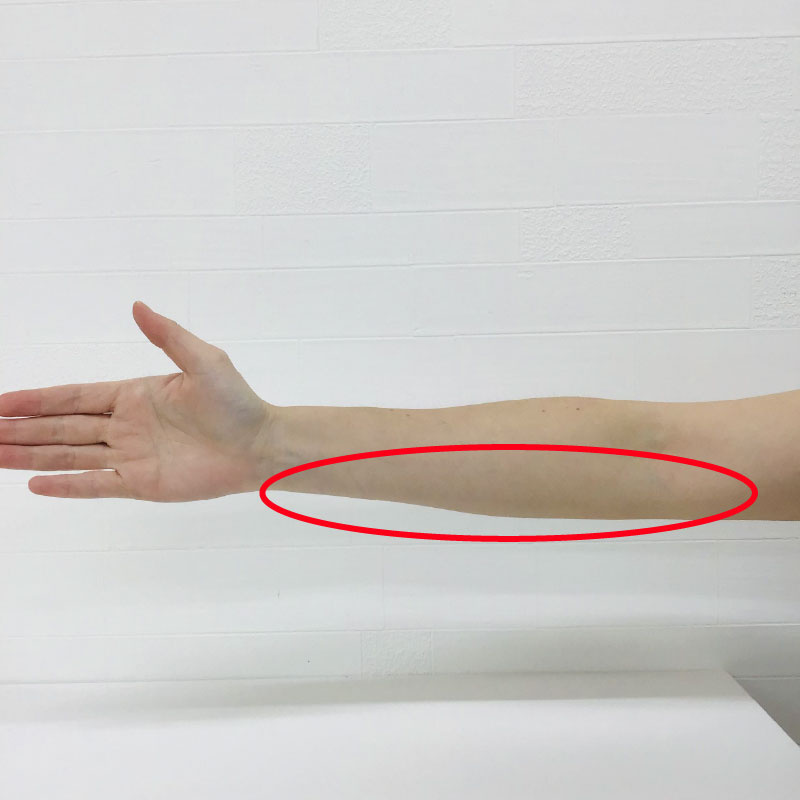
Forearm massage
The muscles connected to the inner (medial) side of the elbow are often tight. When these muscles become stiff, the load on the painful area increases and can worsen symptoms. Massage the area centered around the region marked with a red circle to help relax and soften the muscles. When performing the massage, the use of body cream or body oil is also recommended.
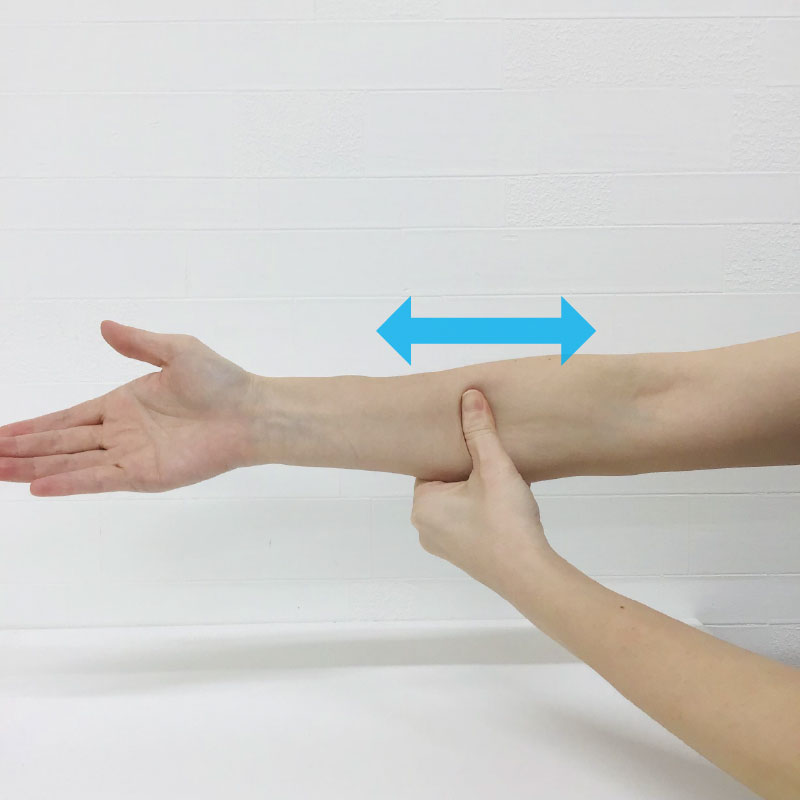
1.Using the opposite hand, pinch the muscles on the little-finger side of the forearm (between the elbow and the wrist). Gently massage while slightly pulling the muscle in the direction of the arrow. Gradually change the area being pulled and massaged to cover the entire region. This massage can also be performed with the elbow bent.
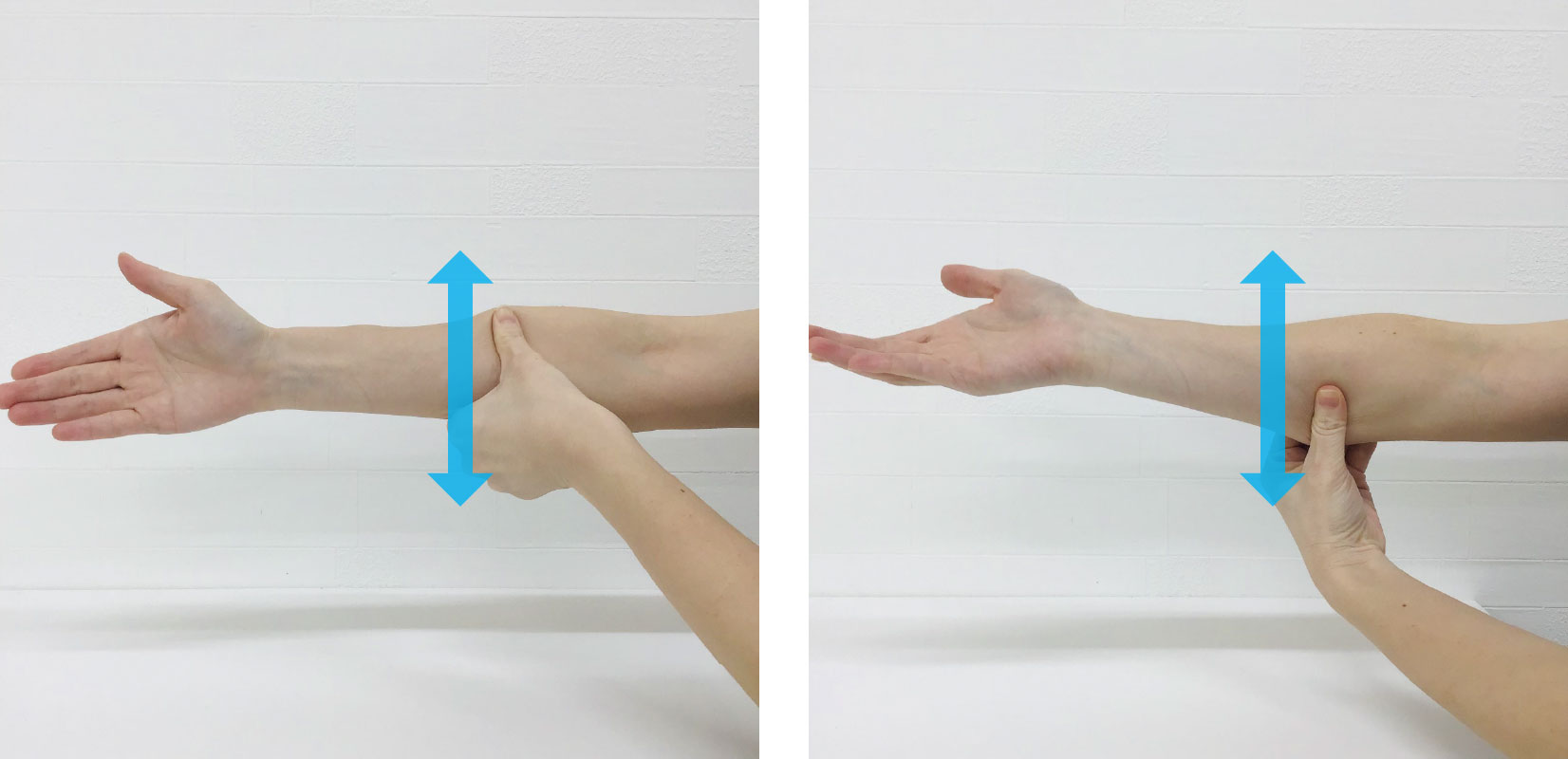
2.As shown in the photograph, place the thumb of the opposite hand on the palm side of the forearm. While gently applying pressure with the thumb, massage by moving it in the direction of the arrow. Gradually change the position and massage the entire area.
3.As shown in the photograph, place the thumb of the opposite hand on the palm side of the forearm. Gently press on the muscle with the thumb while moving it in the direction of the arrow to massage the area. Gradually change the position and massage the entire region.
Consultation
Stretching and massage have not relieved my golfer’s elbow. Are there other treatment options available?
In medial epicondylitis, which is the underlying cause of golfer’s elbow pain, abnormal blood vessels may proliferate. Nerves often grow alongside these abnormal vessels, contributing to persistent pain. In recent years, a new outpatient treatment known as catheter-based therapy has been developed to reduce these abnormal blood vessels. This approach directly targets the abnormal neovascularization that is responsible for prolonged pain.
For more information about our newly introduced Arterial Injection Treatment, please refer to the following link: